A Holistic Review of Lamotrigine: Pharmacological Properties, Therapeutic Applications, and Potential Toxicity
-
Areeba Ajmal
Department of Biotechnology, Institute of Biochemistry, Biotechnology and Bioinformatics, The Islamia University of Bahawalpur, 63100, Punjab, Pakistan
Fatima Ismail

Department of Biotechnology, Institute of Biochemistry, Biotechnology and Bioinformatics, The Islamia University of Bahawalpur, 63100, Punjab, Pakistan
Ayesha SafdarDepartment of Biochemistry and Molecular Biology, Institute of Biochemistry, Biotechnology and Bioinformatics, The Islamia University of Bahawalpur, 63100, Punjab, Pakistan
| Received 03 Jan, 2026 |
Accepted 16 May, 2026 |
Published 30 Jun, 2026 |
Lamotrigine is a phenyltriazine derivative widely used as an anticonvulsant and mood stabilizer for the management of epilepsy and bipolar disorder. It acts primarily by inhibiting voltage-gated sodium channels, thereby reducing excessive neuronal excitability and suppressing the release of excitatory neurotransmitters such as glutamate and aspartate. Lamotrigine undergoes hepatic metabolism mainly through glucuronidation, producing inactive metabolites excreted in urine. Genetic variability in drug-metabolizing enzymes may influence its plasma concentration and therapeutic response. This review comprehensively summarizes the pharmacokinetic and pharmacodynamic properties of lamotrigine, including its absorption, distribution, metabolism, and excretion, along with its clinical applications and toxicity profile. Understanding these aspects is essential for optimizing therapeutic efficacy, minimizing adverse effects, and supporting individualized treatment strategies.
| Copyright © 2026 Ajmal et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Lamotrigine (LTG), as a practical consequence of the theory that there was a connection among the antifolate responses to antiepileptic agents and their efficacy as medicines, serves as a tolerated, effective anticonvulsant medication, licensed for the therapy of acute and generalizing epilepsy in elderly individuals, and in people who have epilepsy with depression or anxiety. It endures significant metabolism and is mostly removed via the kidney, with 94% of the amount supplied orally excreted in urination and 2% in feces. Contingent LTG is responsible about 10% of the chemical compounds detected in your urine. Additionally, there is not a need for a comprehensive description demonstrating the vital role of LTG, which is the therapy of two critical issues: Epileptic seizures and bipolar disorder. It is what is referred to as a “stand-alone” medicament. An analysis of lamotrigine from 2012 embraces all of its characteristics as of that time1.
Graphical Abstract
However, the way that LTG works is similar to the function of phenytoin and carbamazepine. All three medications work by obstructing voltage-dependent Na+ channels, which extends their inactivated mode and stabilizes the postsynaptic membrane Fig. 1. As therefore, Lamotrigine specifically inhibits the discharge of neurotransmitters that stimulate neurons. Over the defined span of plasma concentrations, LTG’s kinetics are constant. After oral dosage, the level of bioavailability is around 100%, and its protein binding is about 50%. The existence or lack of concurrent enzyme-inducing factors or inhibitors affects its clearance (and consequently, terminal half-life). The time it takes to decay rises from around one day to up to 60 hours when valproic acid (VPA) inhibits the enzyme, but it decreases to about 15 hours when inducers such as PHT, CBZ, and phenobarbital (PHB) are used. Hepatically, LTG is converted to N-2- and N-5-glucuronides (80% and 10%, accordingly) as well as other trace amounts of N-oxide, 70% of which are found in urination. Along with clinical concerns (which are discussed here), the following queries were posed:
| • | Information regarding LTG dose and concurrent treatment | |
| • | The degree of seizures, toxicity, marketing or regulatory agencies’ dose recommendations, reported test results and variety of therapies, previous interaction among people on lamotrigine, and input from patients are some of the factors that influence the choice of LTG dosage | |
| • | The effectiveness and suitability of the “therapeutic range” that produced outcomes. Physicians were prompted to choose between “wrong”, “not beneficial”, “beneficial”, and “very beneficial”. Rating levels, which allow you to check boxes, were utilized whenever practical to make answering questions and gathering data easier |
In order to examine the patterns of lamotrigine levels throughout the “therapeutic range” and the extension study to the above analysis was carried out to identify the range of LTG levels determined from 150 consecutive specimens during the initial year of the service and another 150 tested more recently in order to see whether there have been alterations in the amount used medically during this time (i.e., two years after the service was introduced). LTG levels were obtained through a specific HPLC/UV approach that has been reported. In general, the basified plasma portion is extracted into ethyl acetate, then split up, dried, and restored in acetonitrile.
|
Chromatographic separation was carried out on a silica column using a mobile phase of methanol/water/phosphate buffer and monitored by the absorption of ultraviolet light at 280 nm. The approaches had between and within-run coefficients of variation (CV) of 8% or less, and accuracy was controlled via intra bi-level samples for ensuring quality analyzed concurrently, as well as from outside through a worldwide quality assurance system (Heath Control, Cardiff, Wales), where competency has proven constantly appropriate2,3. LTG is a drug used to deal with epilepsy by preventing and managing seizures. Lamotrigine has recently gained popularity because of its clinical manifestations and calming hyperactive impulses in the body. This analysis deeply demonstrates lamotrigine’s therapeutic potential in epilepsy and bipolar disorder, focusing on its clinical effectiveness, safety profile, and usage over time. This analysis comprises a description of key side effects and the accompanying clinical and medical monitoring considerations.
PHARMACOKINETICS
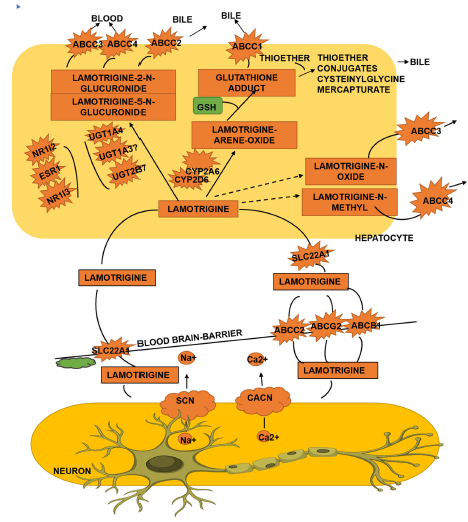
LTG has a nearly 100% bioavailability and is readily absorbed when taken through oral tradition. At adequate dosage, it experiences first-order kinetics. After oral treatment, the highest concentrations happen one to three hours later. The inert N-6 glucuronide conjugate, which is mostly eliminated by the kidneys, is the result of the drug’s liver metabolism. In individuals who are not receiving treatment, the method of elimination of half-life is between 22 and 36 hours. There are tablet and palatable dispersible tablet forms of lamotrigine. When taken orally, lamotrigine is quickly and entirely taken in with minimal digestion during the first pass. Food does not impact its digestion. Individuals with kidney or liver disease have much lower lamotrigine excretion. Lamotrigine pharmacokinetics do not seem to be much impacted by age, gender, or smoking history. Yet, non-whites lamotrigine absorption was 25% lower than whites. The combination of other antiepileptics, especially valproate, is the most important factor influencing lamotrigine absorption. Lamotrigine’s clearance half-life is more than doubled by valproate. Therefore, lamotrigine must be cut in half, and the titration rate decreased if it is administered with valproate4. An exploded visualization of the body’s arrangement of lamotrigine (Fig. 2). Although the exact process by which LTG penetrates the blood–brain barrier (BBB) is unknown, research has suggested that organic cation transporters (OCT) may be involved. LTG is a precursor for SLC22A1 (sometimes referred as OCT1), according to in vitro research, and variations in the SLC22A1 gene have been linked to variations in levels among Chinese epileptic patients.
PHARMACODYNAMICS
The proposed pathway of activity of lamotrigine (Fig. 2). Lamotrigine’s precise mode of action is unknown, but it is most likely due to its antagonistic action on type 2 VGSCs, which are generated by the sodium voltage-gated channel genome family. The mechanism of carbamazepine and phenytoin, two earlier AEDs, is comparable VGSCs are massive proteins that traverse membranes. They have a big alpha subunit that occasionally connects with a smaller regulating beta subunit. When neurological membranes carrying
|
VGSCs are adequately depolarized (usually by an action potential), an alter in the structure of the protein causes the ion pore to open. At the resting stage, the ion pore is in the resting state. Lamotrigine primarily binds to the inactivated mode of VGSCs, functioning as an opposing side, and the channels functionality is said to be inactivated when the inactivation loop blocks the movement of ions through the pore in milliseconds. The docking location for lamotrigine happens to be on the outside of the alpha subunit, which has similarities with carbamazepine and phenytoin. Lamotrigine additionally functions as a contender to high-voltage-activated N-, P-, and Q-type calcium channels (VGCCs) embodied by the calcium voltage-gated channel subunit gene family, which may be another process by which lamotrigine evokes its antiseizure characteristics. VGCCs are physically similar to VGSCs, but they lack the within-cell inactivation loop found in VGSCs. As a result, VGCCs are able to function in an open or closed condition, and they are typically closed at their neutral potential Barring voltage-gated sodium and calcium channels alters the emission of neurotransmitters. Investigations frequently reveal a decline in the excretion of the exuberant neurotransmitter glutamate, followed by lamotrigine delivery.
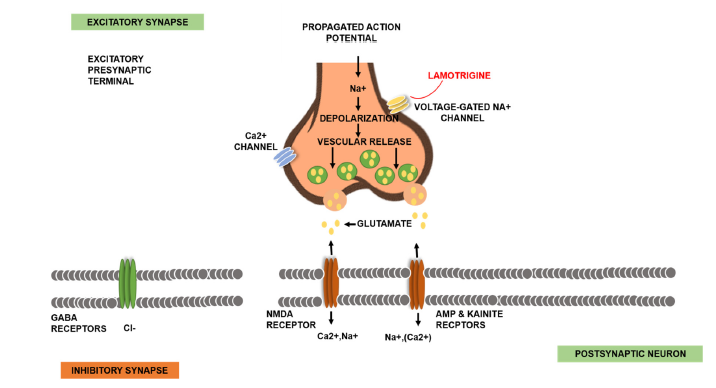
|
However, LTG has been observed to cause both enhanced and reduced emission of restricting neurotransmitter GABA. Calcium’s action as a supplementary messenger inside the cell may potentially cause complex alterations due to changed ion flux. As an illustration, an in vitro investigation employing basic mouse neural cultures discovered that lamotrigine treatment impacted CaM kinase II activity, resulting in changed intracellular calcium contents5.
ABSORPTION, HALF-LIFE AND ELIMINATION ROUTE
Lamotrigine receives adequate absorption after oral treatment and is roughly 55% associated with plasma protein. It underwent a process known as glucuronidation and then elimination through the kidneys, having first-order equations with linear kinetics with an approximate half-life of 24-30 hours. The curative plasma quantity of LTG is predicted to be 1-15 μg/ml, while the hazardous dosage is 16-47 μg/ml. While lamotrigine is substantially converted to glucuronide combines, most writers recommend measuring the parent medication instead of the glucuronide residue (2-N-glucuronide). Several approaches for determining LTG in biological liquids have been published, namely high-efficiency liquid chromatography, liquid chromatography-based tandem mass spectrometry, and gas chromatography-mass spectrometry. Released primarily as a glucuronide combination in the urine. The majority of the medication and its derivatives were retrieved in the urine, with a small amount retrieved in the stool. Urine (65%) and stool (2%).
MECHANISM OF ACTION AND ACTION ON CNS
LTG’s mode effectiveness is complicated as the disruption of sodium channels happens across roughly two kinetic time programs: Rapid and gradual in Fig 3. This medication adheres preferentially to the fast-inactivated condition of channels containing sodium, rather than the slow-inactivated state. It therefore suggests that, at dosages suitable for therapy and substantially destabilized membrane potentials, LTG may effectively block sodium flows by slowly adhering to sodium channels in their fast-inactivated state. This mechanism’s effectiveness relates to phenytoin. LTG and phenytoin have modest bonding rates, which may explain why they are capable of inhibiting seizure outbursts while protecting most ordinary synaptic functions. As a result, LTG has been found to be a successful medication for epilepsy, having an acceptable
| Table 1: | Familiar mechanism of LTG5 | |||
| Mechanism of action | Description | References |
| Infection | Microglia, immune cells found in the brain and spinal cord, are responsible for initiating and maintaining neurological inflammation. LTG has been shown to inhibit stimulation of microglial cells, potentially preventing or reducing neuroinflammation |
Faustmann et al.10 |
| Antioxidant characteristics | LTG exhibits antioxidant capabilities, potentially contributing to its neuroprotective benefits |
Ozkul et al.11 |
| Blockage of sodium channels generally voltage reliant |
LTG inhibits the passage of sodium channels with voltage regulation, lowering the electrical signal in neural networks |
Nakatani et al.12 |
| Modulation by GABA conduction | LTG may boost GABA action, reducing neuronal agitation | Huang et al.13 |
| Reluctance of glutamate emission | LTG reduces the generation of glutamate in the brain, decreasing neurons excitation |
Cunningham and Jones14 |
| LTG: Lamotrigine, GABA: Gamma-aminobutyric acid, All mechanisms are based on experimental and clinical evidence describing the pharmacodynamic actions of lamotrigine | ||
safety record because of its exclusive blockage of rapid inactivated sodium channels7. LTG’s approach, contrasted to other AEDs, might give benefits in controlling specific types of convulsions. LTG operates by restraining voltage-influenced Na+ channels, lowering calcium flows, and blocking the production of specific synapses in the brain, for example, glutamate and aspartate support to its expansive efficiency Such hindering only occurs during episodes of seizures, minimizing negative effects throughout non-seizure periods; nevertheless, its mode of action is not entirely understood5 Additional neurotransmitters, namely serotonin, norepinephrine, and dopamine, do not appear to be appreciably altered by LTG. This regulates the electrical signals in the brain and decreases seizures. In conclusion, the working method may have benefits in controlling seizures caused by glutamate excitation. Various AEDs, with distinct modes of action, may be more efficient at treating multiple kinds of seizures, among them those caused by GABA dysregulation or calcium channel failure. Furthermore, lamotrigine is less likely to cause drowsiness or cognitive decline than some other anti-epileptic medicines, making it suitable for the therapy of a few mood disorders in conjunction with epilepsy8. Known mechanisms of LTG (Table 1)
PHARMACOLOGICAL APPLICATIONS
LAMOTRIGINE ACTION ON THE CARDIOVASCULAR SYSTEM
Lamotrigine has been an increasingly prevalent antiseizure medicine, often doing exceptionally well in contrasting efficacy tests and frequently prescribed for the therapy of seizures in older people15. Furthermore, lamotrigine is regarded as the primary treatment for bipolar disorder An approximate average prevalence of 4.8% in males and 3.6% in females aged 65-74, cardiac arrhythmias are quite common and cardiac arrhythmias contribute 15-20 % of the total fatalities16. Therefore, a higher risk of proarrhythmic effects with lamotrigine has significant ramifications for the management of epileptic and bipolar illness. The FDA’s fall 2020 security guidance, which unexpectedly warned of the possibility of adverse effects via lamotrigine medication for individuals with basic cardiovascular disorders or arrhythmias of the heart, quickly sparked debate and attention among the entire epileptic seizures and behavioral health community17. Additionally, to its activities on the sodium channel, lamotrigine inhibits high-voltage-activated Ca² flows in a dosage-dependent way, most likely by inhibiting N- along with P/Q-type channels for Ca² in the postsynaptic membrane activity. At increased blood levels, lamotrigine may clog K-hERG pathway18. Nav1.5 appears primarily in cardiac tissue and is considered crucial for the destabilization stage of the heart’s contraction state inside the voltage-gated and sodium-gated channels. A medication that largely blocks this pathway may produce arrhythmias; thus, caution is advised. It is observed that LTG can inhibit the Nav1.5 channel, but its effectiveness is limited19. Together with in vitro electrophysiological investigations, results from 54 individuals in good health administered with LTG show that at a dose of fifteen ug/ml, producing PR fluctuations in placebo. Furthermore, while lamotrigine therapy individuals experienced a small decrease of the ventricular depolarization, no participant had a QRS complex longer than 120 ms19.
|
In an ongoing examination of 108 senior people (average age: 73 years) who participated in an independent effectiveness trial among CBZ and LTG, Studies found no major changes in ventricular depolarization between the two therapy groups20. At the stage of examination, the standard daily dose of lamotrigine was 111 ± 33 mg. CBZ (415±143 mg/day) resulted in a small rise in the PR period (170 to 180 ms), was not pertinent to clinical practice clinical. In recent times, various major retrospective analyses sought to answer this topic. In an extensive population-centered cohort research determined that there was nothing to proof associating heart-related fatality or cardiovascular problems roughly 91,000 fresh users of LTG21. The average lifespan of this group of people was younger than those investigated21. At last, Aboukaoud and coworkers searched the Food and Drug Administration’s Hazardous ERS database for the proof of LTG heart related fatalities or arrhythmias. Although there were no significant findings in the epileptic group, people having a mental reason for LTG treatment reported six times more fatal heart events and had higher rates of complaints about cardiac arrhythmia22. Associations between drugs and suicide are both possible explanations for all of these findings. Our findings, based on a more elderly sample of military personnel using LTG to treat seizures and mental health issues, indicate no clear correlation or extra risk between lamotrigine and cardiovascular conduction irregularities. Undoubtedly, all retrospective investigations have inherent drawbacks. While we did not identify a signal indicates that this subject is not completely settled, and an array of patients might actually be in danger23.
NEUROPROTECTIVE ROLE OF LAMOTRIGINE
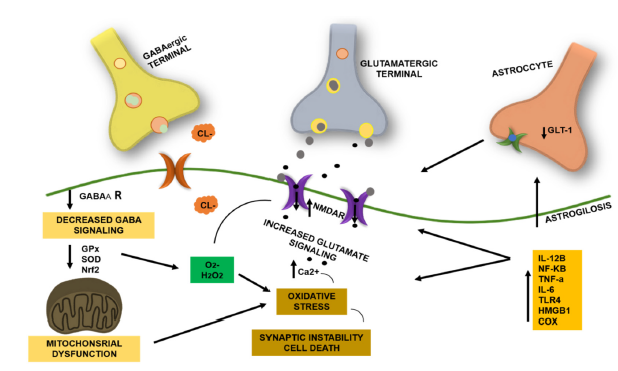
The interruption of standard excitatory transmission of signals monitored by glutamate and its ligand-gated ionotropic receptors known as glutamate contributes to a broad spectrum of pathophysiology of neurological ailments, which include epilepsy, hypoxic-ischemic damage to the brain, and neurodegenerative illnesses such as diseases like Parkinson’s, Alzheimer’s, Huntington’s syndrome, and multiple sclerosis (MS)24. Lamotrigine, aripiprazole, and escitalopram protect against depression-induced oxidative damage. It was revealed that lamotrigine had the highest preventive impact on oxidative damage among the three medications25. After inducing 15 mM glutamate in SH-SY5Y cells, we observed a rise in TNF-α, IL-1β, and IL-6 levels. Lamotrigine greatly reduced this rise in levels. Likewise, to our findings, an Alzheimer’s model using SH-SY5Y cells showed that TNF-α levels elevated following administration with Amyloid-β (Aβ) in Fig. 4. Mechanical trauma injury increases TNF-α and IL-6 levels in the SH-SY5Y cell model. The amounts of inflammatory variables are raised in nerve cells under pathological situations, including a state of ischemia, hypoxemia, mitogens, cytokines, and hormones, resulting in neuronal death26 Glial cells, comprising astrocytes along with microglia, are widely recognized as the primary source of pro-inflammatory cytokines produced in the CNS.
|
In reactions to hazardous stimuli, each glial and neuronal cell has been shown to generate and secrete pro-inflammatory cytokines, which react to chemokines & adhesion molecules. Pro-inflammatory cytokines regulate processes of inflammation27. This analysis found that lamotrigine significantly reduced IL-1β, IL-6, and TNF-α levels within glutamate-exposed cells. Additional studies found that lamotrigine had different impacts on cytokine concentrations. Lamotrigine reduced IL-6 and TNF-α secretion in both in vivo and in vitro lipopolysaccharide/concanavalin A (LPS)-induced inflammatory models, but only in the ConA-induced pathway of IL-1β26. in vitro, lamotrigine inhibited TNF-α and IL-1β secretion but had no impact on IL-6 secretion when entire blood from competent female participants was stimulated with the syndrome of toxic shock toxin-126. Lamotrigine lowered IL-1β secretion, whereas TNF-α and IL-6 levels remained unchanged after stimulation with anti-CD3 and anti-CD40 antibodies. It was believed that the various impacts on the proinflammatory cytokines between the research could be related to changes in the stimulants, cells, and various other experimental scenarios In summary, the findings of this investigation show that lamotrigine has neuroprotective benefits towards glutamate26.
ANTICANCER ROLE OF LAMOTRIGINE
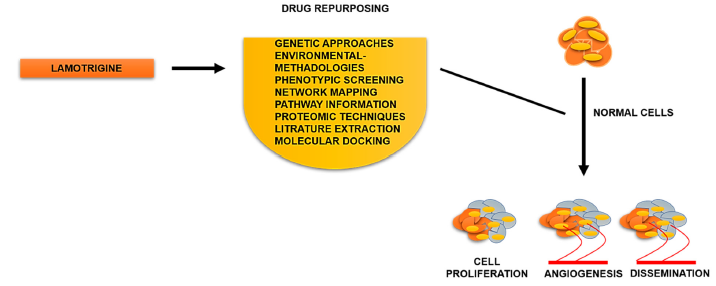
Lamotrigine is not effective towards cervical or breast cancer in Fig. 5. Furthermore, it does not have antibacterial properties. According to previous findings, quaternary ammonium salts exhibit antimicrobial and cancer-fighting abilities. Our goal was to insert a cationic benzyl group in the triazine ring of lamotrigine to increase its ability to interact with microbial and cancer target regions29. Lamotrigine, similar to lacosamide, is a promising prospective add-on drug for tumors in brain patients via proliferation of cells and death, inhibiting cell migrations and invasions30.
INTERACTION OF LAMOTRIGINE WITH OTHER DRUGS
Clinical data indicate that specific AED formulations may be related to harmful or favorable interactions at the pharmacodynamic level. The combined use of valproate and lamotrigine or valproate and ethosuximide has often been demonstrated to be exceptionally successful in causing epileptic control in patients who were unresponsive to the maximal acceptable amount of either drug administered by itself. This phenomenon might be explained by a pharmaceutical connection leading to mutual ineffectiveness or inducing harm to the brain31.
| Table2: | The clinical indications of exposure to lamotrigine38 | |||
| Clinical Impact | n (%) | Clinical Impact | n (%) |
| Trembling | 9 (1.8) | Queasiness | 25 (5.1) |
| Garbled speech | 9 (1.8) | Emesis | 54 (11) |
| Eruption | 9 (1.8) | Fatigue | 103 (20.9) |
| Uncontrolled eye motion | 8 (1.6) | Stumbling | 24 (4.9) |
| Palpitations | 22 (4.5) | Unconsciousness | 6 (1.2) |
| Wooziness | 22 (4.5) | Convulsions | 8 (1.6) |
| Restlessness | 11 (2.2) | Hazy vision | 7 (1.4) |
| Disorientation | 10 (2.0) | ||
| n: Number of reported cases; %: Percentage of total cases, Clinical effects represent commonly reported adverse reactions associated with lamotrigine use. Percentages are based on the total study population | |||
Carbamazepine, lamotrigine, and oxcarbazepine have been linked to higher neurotoxic effects than combinations of the same medicines with other agents, which could be accounted for by carbamazepine’s common function in obstructing voltage-dependent sodium channels. Actually, combinations of medications working by different means would be predicted to be more helpful than combinations of medications having a similar mechanism of action. However, present understanding of the pharmacology of AEDs is currently inadequate to enable a mechanistic strategy for AED treatment32. The Lamotrigine blood plasma dose to level ratio (LTG-CDR) is 14.8 (9.9-24.6) (ng/mL)/(mg/day). A standard mixed technique, which allows for several recordings from an identical patient, was used to identify and quantify the effect of different variables influencing the LTG-CDR. In addition to chronological age and gender, 35 different medicines (25 mental and 5-10 others) were investigated. With women under the age of 70 as the reference group, male gender and treatment with ethinylestradiol, carbamazepine, lithium, fluoxetine, phenobarbital, phenytoin, and topiramate resulted in significantly lower LTG-CDR. Age under seventy years and combined treatment with valproate were associated with significantly higher LTG-CDR levels. Apart from fluoxetine, no antidepressants or antipsychotic medications were found to modify the LTG-CDR. Regarding pharmacokinetic medication interactions, we find that lamotrigine can be used effectively coupled with major psychiatric medicines33.
LAMOTRIGINE SIDE EFFECTS
In the elderly, vision problems, dizziness, diplopia, fainting, gastrointestinal issues (diarrhea, nausea, or abdominal discomfort), tremors, and headaches are the most often reported side effects experienced after chronic lamotrigine treatment. Among the most often mentioned negative effects in children are rash and somnolence, which are primarily experienced by valproate users, and exacerbated responses, which are primarily experienced by patients taking enzyme-inducing drugs. Vertigo, ataxia, headaches, vomiting, diplopia, and irritation were also observed in as many as 19% of children using lamotrigine. Other than rash, no reports of potentially dangerous reactions were made until lately34. Twelve supervised bipolar clinical trials showed tremor (3.9%), diarrhea (6.2%), and dry mouth (6.3%) as additional, comparatively less frequent side effects. According to data from bipolar clinical trials, 2.5% of 1256 patients receiving lamotrigine experienced the serious adverse events of mania, hypomania, and mixed mania; however, this was thought to be similar to the rate observed in patients receiving placebo (2.2% of 1094 patients) and lithium (2.5% of 280 patients taking them). According to the research, lamotrigine was linked to a 0.5% probability of these side effects35. Mental illnesses are linked to a higher risk of suicidal behavior, with self-poisoning being a prevalent approach, resulting in 20.2% (N ≈ 1259) and 38.2% (N ≈ 2381) of female and male suicides in the UK in 2013. Even when no other mental disorders are present, epilepsy has been associated to an elevated possibility of suicide. As a result, people administered lamotrigine are possibly at higher risk of intentional overdose from drugs36. The scientific proof for the hazardous consequences of lamotrigine in dosage is primarily based on certain case reports, the majority of which focus on a number of particular aspects unique to the instance in question. Given the known and increasing use of lamotrigine in categories of patients who are at a higher risk of drug overdose, prescribers want information on its safety record in overdose when weighing the risks and advantages of its usage. Thus, we conducted a study of the literature to synthesize the available information on the protective behavior of lamotrigine in overdose37. Indications of LTG (Table. 2).
|
LTG INDUCED TOXICITY
HEPATOTOXICITY
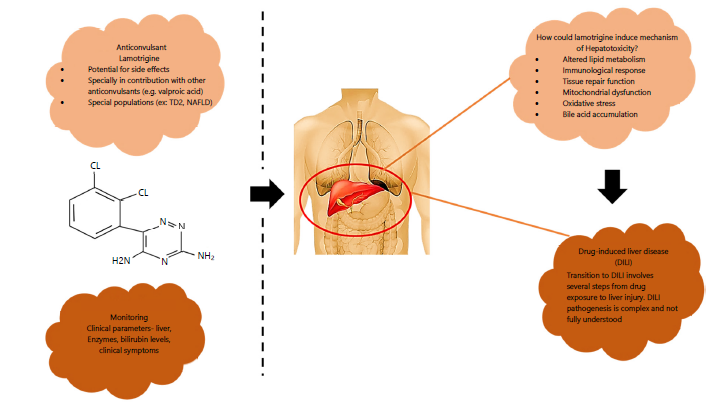
Hepatotoxicity caused by lamotrigine is quite uncommon, but it can develop and escalate to drug-induced liver injury (DILI). DILI is a major clinical concern that has garnered more scrutiny in the past few decades due to its capability to create serious health difficulties and its status as one of the most prevalent and dangerous adverse medication reactions. The first step in treating DILI is to stop using the substance or prescription that is causing it. However, optimal care requires a comprehensive therapeutic approach that includes both pharmaceutical therapies and supporting measures. DILI’s complex pathophysiology and lack of specific diagnostic markers make it difficult to diagnose39. Symptoms of lamotrigine-induced hepatotoxicity include jaundice, increased transaminases, and multisystem involvement, which includes renal failure and disseminated intravascular coagulation. This undesirable reaction is more likely to occur in some patient groups, especially those with Type 2 Diabetes (TD2) and Non-Alcoholic Fatty Liver Disease (NAFLD)40 The presentation and outcome of DILI are impacted by the simultaneous existence of TD2 and NAFLD, with NAFLD increased vulnerability to DILI by causing alterations in the hepatic absorption, distribution, metabolism, and transfer of xenobiotics. A greater potential of hepatotoxicity has been associated with higher dosages and abrupt escalation of lamotrigine. In order to offer substantial knowledge into the mechanisms causing DILI, we examine the consequences of excessive medication dosages, or levels outside of the therapeutic range. Excessive use increases the drug’s pharmacological impacts, revealing pathways that lead to liver injury. An overdose can activate the immune system, causing inflammation as well as harm to liver cells. This helps identify critical proteins and pathways implicated in the drug’s hepatotoxicity. Unlike carbamazepine, genetic studies have found no significant link between specific variations and lamotrigine-induced liver injury. The insufficient awareness of the processes behind lamotrigine’s action, which is critical for its therapeutic effects, creates unique hurdles, particularly in interpreting negative consequences such as DILI or cardiac issues (Fig. 6). This sophisticated knowledge may not affect dosage modifications, but it could complicate the evaluation of possible side effects. Dosing practices differ depending on the ailment, necessitating close supervision by healthcare specialists40.
Illustration of how the anticonvulsant lamotrigine interacts with the possible hepatotoxic risk and the importance of monitoring. In addition to providing a visual aid to improve comprehension, the figure highlights the importance of being vigilant in monitoring for the best possible safety of patients and therapeutic results40.
TERATOGENICITY
Infants of women who administered lamotrigine during the initial twelve weeks of pregnancy were more likely to have poor fetal development. The study on mice found that lamotrigine was probably an ignition point for the emergence of bone defects in the developing infant of mice given lamotrigine during pregnancy. That is to say, abnormalities in the bones were recorded in some of these newborns, even when defects that contributed to stillbirth were not found; nonetheless, the frequency was reduced compared to that of other medicines, such as sodium valproate. In accordance with the investigation’s outcomes, newborns born to mothers who consumed lamotrigine while expecting were significantly shorter than those born to both control and carrier individuals. The median lifespan of newborns with mothers who were administered lamotrigine medication decreased considerably due to the effects of lamotrigine on rodents41. Thus, prior research indicates that infants whose mothers consumed lamotrigine during pregnancy are more likely than the general population to have low birth weight and skeletal deformities; these findings are in line with the latest research. Significant harm to the babies’ gonadal tissue was evident from the significantly decreased number of oocytes in the lamotrigine group compared to the control and vehicle groups. As previously mentioned, no research was done to examine how lamotrigine affected the infant’s gonads. On the other hand, the quantity of oocytes and secondary follicles in the group that was receiving the drug considerably decreased when compared to the control group. This analysis examined the long-term therapeutic consequences (90 days) of 5 mg lamotrigine on adult female rats42. Therefore, by decreasing oocytes and follicles of the ovaries, lamotrigine appears to produce early ovarian failure and decreased fertility in fetuses whose mothers received the drug, similar to what happens with adult rats. During the early stages of pregnancy, lamotrigine can cross the placenta, apply its toxicity to the gonads, and ultimately impact future fertility rates. The findings demonstrated that giving pregnant women 20 mg of lamotrigine may harm the developing fetus’s gonads. To put it another way, lamotrigine appears to lower reproduction capability by directly harming male fetuses’ seminiferous tubules and decreasing the quantity of oocytes in female fetuses41.
REPROTOXICITY
On gestation day (GD) 7 or 8, groups of TO mice received a single (50-200 mg/kg) or several doses (25, 50, 75 mg/kg) of LTG via intraperitoneal (i.e., injection) (notice that the treatment is oral). The embryos were obtained on GD 18. The LTG-treated group had maternal toxic effects such as dose-related mortality, higher abortion rates, fetal death, congenital anomalies, or intrauterine growth retardation (IUGR). The treatment of LTG in many small amounts contributed to enhanced mother morbidity and a greater percentage of amniotic disintegration and anomalies as the amount administered progressed; IUGR was significant but dose independent. Several low-dose group infants displayed anomalies, including maxillary-mandibular hypoplasia, exencephaly, palate defects, median facial defect, genital anomalies, and varying degrees of caudal regression. This suggests that LTG delivered i.e. at high doses can cause intrauterine growth retardation, whilst modest repeated doses cause a dose-dependent rise in embryonic resorption, craniofacial and caudal abnormalities, and maternal toxicity in the mouse. Previous research in other laboratories using the oral route of exposure found that there were no teratogenic consequences associated with LTG dosages that are not maternally toxic42,43.
NEPHROTOXICITY
DRESS syndrome considered a particularly relevant diagnosis after determining that LTG is a known cause of cutaneous side effects. Between 13 and 35% of people with internal organ injury had renal involvement during DRESS syndrome. Although the precise cause is yet unknown, kidney damage in DRESS syndrome is frequently linked to AIN (typical triad: rash, eosinophilia, fever). Drug-triggered acute interstitial nephritis and, even more interestingly, DRESS are thought to be caused by an idiosyncratic prolonged type IV hypersensitivity response. It starts with the emergence of events that trigger an inner cell immune system reaction either by causing immediate cellular harm or by releasing antibodies44. In earlier times, DRESS and chronic interstitial nephritis were classified as distinct clinical illnesses, despite similar symptoms like a rash, fever, and a possible shared cause. Therefore, we advise creating a uniform category, preferably centered around its origin, for drug-associated illnesses, including damage to the kidneys. In our case, study showed interstitial nephritis and tubular necrosis, demonstrating severe acute interstitial nephritis with a tubular necrotic component, which is consistent with findings in previous DRESS patients with renal involvement. Acute interstitial nephritis and DRESS, as opposed to acute tubular necrosis, are regarded as dosage reliant. On the other hand, in our patient, we believe that inability to follow prescribed antiepileptic drug doses, which resulted in variable and sometimes increased drug levels, contributed to renal failure. The possibility of a rash with lamotrigine has been shown to rise if the first dosage or increase in dose rate is surpassed. In this section, both are applicable45. In the lack of controlled research, suggestions for therapy for DRESS rely on empirical and consensus-based techniques that mostly involve systemic corticosteroids reduced over three months. Extended outlook has not been reported consistently. The originally normal lamotrigine levels were deceiving in the diagnosis process. This report seeks to improve awareness of the common hazards of therapy noncompliance in the pediatric community. Roughly 50% of youngsters are found to not adhere to therapy protocols, and this number tends to increase throughout puberty. We postulate that lamotrigine overdose causes acute renal injury via AIN in combination with ATN as part of DRESS or HSS. When analyzing drug-induced negative impacts in pediatric individuals, non-compliance may exist despite the dosages falling within the typical range of values45.
CONCLUSION
Lamotrigine is an effective anticonvulsant and mood stabilizer with a favorable safety and cognitive profile. Its therapeutic efficacy is primarily linked to modulation of sodium channels and neurotransmitter release. However, risks such as hepatotoxicity, dermatological reactions, and potential cardiac effects necessitate careful dose titration and monitoring. A thorough understanding of its pharmacological properties is essential to ensure safe and optimized clinical use.
SIGNIFICANCE STATEMENT
Lamotrigine is a widely used anticonvulsant and mood stabilizer with significant clinical importance in managing epilepsy and bipolar disorder. Understanding its pharmacokinetics and pharmacodynamics is essential for optimizing therapeutic efficacy and minimizing adverse effects. This review highlights key mechanisms, metabolic variability, and safety considerations, providing valuable insights for clinicians to enhance personalized treatment strategies and improve patient outcomes.
REFERENCES
- Żełabowski, K., K. Wojtysiak, Z. Ratka, K. Biedka and A. Chłopaś-Konowałek, 2025. Lamotrigine therapy: Relation between treatment of bipolar affective disorder and incidence of Stevens-Johnson syndrome-a narrative review of the existing literature. J. Clin. Med., 14.
- Gupta, D., S.K. Shrivastava and R.K. Malviya, 2022. Preformulation studies of lamotrigine. NeuroQuantology, 20: 1357-1369.
- Morris, R.G., M.Y.Y. Lee, X. Cleanthous and A.B. Black, 2004. Long-term follow-up using a higher target range for lamotrigine monitoring. Ther. Drug Monit., 26: 626-632.
- Grasela, T.H., J. Fiedler-Kelly, E. Cox, G.P. Womble, M.E. Risner and C. Chen, 1999. Population pharmacokinetics of lamotrigine adjunctive therapy in adults with epilepsy. J. Clin. Pharmacol., 39: 373-384.
- Costa, B. and N. Vale, 2023. Understanding lamotrigine’s role in the CNS and possible future evolution. Int. J. Mol. Sci., 24.
- Chan, V., R.G. Morris, K.F. Ilett and S.E. Tett, 2001. Population pharmacokinetics of lamotrigine. Ther. Drug Monit., 23: 630-635.
- Yang, H., D. Zhang, S. Wei, Z. Zhao and S. Mei, 2024. Population pharmacokinetics of lamotrigine and its N2-glucuronide metabolite in Chinese patients with epilepsy. Ther. Drug Monit., 46: 649-657.
- Li, C., X. Wang, M. Deng, Q. Luo and C. Yang et al., 2025. Antiepileptic drug combinations for epilepsy: Mechanisms, clinical strategies, and future prospects. Int. J. Mol. Sci., 26.
- Löscher, W., M. Gillard, Z.A. Sands, R.M. Kaminski and H. Klitgaard, 2016. Synaptic vesicle glycoprotein 2A ligands in the treatment of epilepsy and beyond. CNS Drugs, 30: 1055-1077.
- Faustmann, T.J., F. Corvace, P.M. Faustmann and F.S. Ismail, 2022. Effects of lamotrigine and topiramate on glial properties in an astrocyte-microglia co-culture model of inflammation. Int. J. Neuropsychopharmacol., 25: 185-196.
- Ozkul, A., A. Sair, A. Akyol, C. Yenisey, T. Dost and C. Tataroglu, 2014. Effects of lithium and lamotrigine on oxidative-nitrosative stress and spatial learning deficit after global cerebral ischemia. Neurochem. Res., 39: 853-861.
- Nakatani, Y., H. Masuko and T. Amano, 2013. The effect of lamotrigine on Nav1.4 voltage-gated sodium channels. J. Pharmacol. Sci., 123: 203-206.
- Huang, Y.Y., Y.C. Liu, C.T. Lee, Y.C. Lin and M.L. Wang et al., 2016. Revisiting the lamotrigine-mediated effect on hippocampal GABAergic transmission. Int. J. Mol. Sci., 17.
- Cunningham, M.O. and R.S.G. Jones, 2000. The anticonvulsant, lamotrigine decreases spontaneous glutamate release but increases spontaneous GABA release in the rat entorhinal cortex in vitro. Neuropharmacology, 39: 2139-2146.
- Arif, H., R. Buchsbaum, J. Pierro, M. Whalen and J. Sims et al., 2010. Comparative effectiveness of 10 antiepileptic drugs in older adults with epilepsy. Arch. Neurol., 67: 408-415.
- >Haenen, N., A.M. Kamperman, A. Prodan, W.A. Nolen, M.P. Boks and R. Wesseloo, 2024. The efficacy of lamotrigine in bipolar disorder: A systematic review and meta-analysis. Bipolar Disord., 26: 431-441.
- Restrepo, J.A., R.L. MacLean, C.M. Celano, J.C. Huffman, J.L. Januzzi and S.R. Beach, 2022. The assessment of cardiac risk in patients taking lamotrigine; a systematic review. Gen. Hosp. Psychiatry, 78: 14-27.
- Danielsson, B.R., K. Lansdell, L. Patmore and T. Tomson, 2005. Effects of the antiepileptic drugs lamotrigine, topiramate and gabapentin on hERG potassium currents. Epilepsy Res., 63: 17-25.
- Ingleby-Talecki, L., S.C. van Dijkman, S.P. Oosterholt, O.D. Pasqua and C. Winter et al., 2022. Cardiac sodium channel inhibition by lamotrigine: In vitro characterization and clinical implications. Clin. Transl. Sci., 15: 1978-1989.
- Saetre, E., E. Perucca, J. Isojärvi and L. Gjerstad, 2007. An international multicenter randomized double-blind controlled trial of lamotrigine and sustained-release carbamazepine in the treatment of newly diagnosed epilepsy in the elderly. Epilepsia, 48: 1292-1302.
- Christensen, J., B.B. Trabjerg and J.W. Dreier, 2022. Cardiac morbidity and mortality associated with the use of lamotrigine. Epilepsia, 63: 2371-2380.
- Aboukaoud, M., A. Wilf-Yarkoni and E. Maor, 2023. Investigation of cardiac arrhythmia events in patients treated with lamotrigine: FDA adverse event reporing system analysis. Epilepsia, 64: 2322-2329.
- Biehl, A., M. Taube, R.J. Kotloski, K. Kopacek, J. Jones and B.E. Gidal, 2023. Lamotrigine use and potential for adverse cardiac effects: A retrospective evaluation in a Veteran population. Epilepsy Behav., 149.
- Teleanu, R.I., A.G. Niculescu, E. Roza, O. Vladâcenco, A.M. Grumezescu and D.M. Teleanu, 2022. Neurotransmitters-key factors in neurological and neurodegenerative disorders of the central nervous system. Int. J. Mol. Sci., 23.
- Eren, I., M. Naziroglu and A. Demirdas, 2007. Protective effects of lamotrigine, aripiprazole and escitalopram on depression-induced oxidative stress in rat brain. Neurochem. Res., 32: 1188-1195.
- Bebıtoglu, B.T., E. Oguz, N.G. Acet, A. Hodzıc, F. Temel, S. Ada and A. Kılıckap, 2020. The neuroprotective effect of lamotrigine against glutamate excitotoxicity in SH-SY5Y human neuroblastoma cells. Marmara Med. J., 33: 146-152.
- Rosales-Corral, S., R.J. Reiter, D.X. Tan, G.G. Ortiz and G. Lopez-Armas, 2010. Functional aspects of redox control during neuroinflammation. Antioxid. Redox Signaling, 13: 193-247.
- Parsons, A.L.M., E.M.V. Bucknor, E. Castroflorio, T.R. Soares, P.L. Oliver and D. Rial, 2022. The interconnected mechanisms of oxidative stress and neuroinflammation in epilepsy. Antioxidants, 11.
- Khan, M.K., H. Siddiqui, R. Sharif, M. Guzel, Atia-tul Wahab, S. Yousuf and M.I. Choudhary, 2022. Lamotrigine derivatives-synthesis, anti-cancer, and anti-MDR-bacterial activities. J. Mol. Struct., 1264.
- Aroosa, M., J.A. Malik, S. Ahmed, O. Bender, N. Ahemad and S. Anwar, 2023. The evidence for repurposing anti-epileptic drugs to target cancer. Mol. Biol. Rep., 50: 7667-7680.
- Taing, K.D., T.J. O’Brien, D.A. Williams and C.R. French, 2017. Anti-epileptic drug combination efficacy in an in vitro seizure model-phenytoin and valproate, lamotrigine and valproate. PLoS ONE, 12.
- Perucca, E., 2006. Clinically relevant drug interactions with antiepileptic drugs. Br. J. Clin. Pharmacol., 61: 246-255.
- Reimers, A., E. Skogvoll, J.K. Sund and O. Spigset, 2005. Drug interactions between lamotrigine and psychoactive drugs. J. Clin. Psychopharmacol., 25: 342-348.
- Fayad, M., R. Choueiri and M. Mikati, 2000. Potential hepatotoxicity of lamotrigine. Pediatr. Neurol., 22: 49-52.
- Seo, H.J., A. Chiesa, S.J. Lee, A.A. Patkar and C. Han et al., 2011. Safety and tolerability of lamotrigine: Results from 12 placebo-controlled clinical trials and clinical implications. Clin. Neuropharmacol., 34: 39-47.
- Christensen, J., M. Vestergaard, P.B. Mortensen, P. Sidenius and E. Agerbo, 2007. Epilepsy and risk of suicide: A population-based case-control study. Lancet Neurol., 6: 693-698.
- Alabi, A., A. Todd, A. Husband and J. Reilly, 2016. Safety profile of lamotrigine in overdose. Ther. Adv. Psychopharmacol., 6: 369-381.
- Lofton, A.L. and W. Klein-Schwartz, 2004. Evaluation of lamotrigine toxicity reported to poison centers. Ann. Pharmacother., 38: 1811-1815.
- Im, S.G., S.H. Yoo, Y.M. Park, S.J. Lee and S.K. Jang et al., 2015. Liver dysfunction induced by systemic hypersensitivity reaction to lamotrigine: Case report. Clin. Mol. Hepatol., 21: 180-182.
- Costa, B., I. Silva, J.C. Oliveira, H. Reguengo and N. Vale, 2024. Pharmacokinetic simulation study: Exploring the impact of clinical parameters on lamotrigine for different patient populations with implications for liver function assessment and therapeutic drug monitoring. Sci. Pharm., 92.
- Sathiya, S., M. Ganesh, P. Kalaivani, V. Ranju, S. Janani, B. Pramila and C.S. Babu, 2014. Prenatal exposure to lamotrigine: Effects on postnatal development and behaviour in rat offspring. Int. Scholarly Res. Not., 2014.
- Røste, L.S., E. Taubøll, J.I.T Isojärvi, A. Berner and K.A. Berg et al., 2003. Gonadal morphology and sex hormones in male and female Wistar rats after long-term lamotrigine treatment. Seizure, 12: 621-627.
- Padmanabhan, R., Y.M. Abdulrazzaq, S.M.A. Bastaki, M. Shafiullah and S.I. Chandranath, 2003. Experimental studies on reproductive toxicologic effects of lamotrigine in mice. Birth Defects Res. Part B: Dev. Reprod. Toxicol., 68: 428-438.
- Brüning, K.K., E. Pelivan, M.C. Heinrich, P. Bufler, A. Kaindl and J. Thumfart, 2024. Acute kidney injury in lamotrigine-induced DRESS syndrome. Pediatr. Nephrol., 39: 3213-3215.
- da Silva, M.D., S.M. Domingues, S. Oluic, M. Radovanovic and P. Kodela et al., 2023. Renal manifestations of drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: A systematic review of 71 cases. J. Clin. Med., 12.
How to Cite this paper?
APA-7 Style
Ajmal,
A., Ismail,
F., Safdar,
A. (2026). A Holistic Review of Lamotrigine: Pharmacological Properties, Therapeutic Applications, and Potential Toxicity. Trends in Pharmacology and Toxicology, 2(2), 72-85. https://doi.org/10.21124/tpt.2026.72.85
ACS Style
Ajmal,
A.; Ismail,
F.; Safdar,
A. A Holistic Review of Lamotrigine: Pharmacological Properties, Therapeutic Applications, and Potential Toxicity. Trends Pharm. Toxicol. 2026, 2, 72-85. https://doi.org/10.21124/tpt.2026.72.85
AMA Style
Ajmal
A, Ismail
F, Safdar
A. A Holistic Review of Lamotrigine: Pharmacological Properties, Therapeutic Applications, and Potential Toxicity. Trends in Pharmacology and Toxicology. 2026; 2(2): 72-85. https://doi.org/10.21124/tpt.2026.72.85
Chicago/Turabian Style
Ajmal, Areeba, Fatima Ismail, and Ayesha Safdar.
2026. "A Holistic Review of Lamotrigine: Pharmacological Properties, Therapeutic Applications, and Potential Toxicity" Trends in Pharmacology and Toxicology 2, no. 2: 72-85. https://doi.org/10.21124/tpt.2026.72.85

This work is licensed under a Creative Commons Attribution 4.0 International License.